ST Elevation vs Non-ST Elevation Myocardial Infarction (STEMI vs NSTEMI)
Description: Learn the practical ECG, troponin, and clinical differences between STEMI and NSTEMI, including why ECG timing, serial testing, and early recognition matter in acute coronary syndrome.

|
Quick answer: STEMI and NSTEMI are both acute myocardial infarctions, but STEMI usually presents with persistent ST-segment elevation on the ECG and typically reflects a more abrupt complete coronary occlusion requiring immediate reperfusion. NSTEMI does not show persistent ST elevation, usually reflects subendocardial infarction, and is diagnosed using symptoms, ECG findings such as ST depression or T-wave inversion, and a rise and/or fall in troponin above the 99th percentile with evidence of ischaemia. |
One of the most important early distinctions in acute cardiology is the difference between ST-elevation myocardial infarction and non-ST-elevation myocardial infarction. For medical students and junior doctors, this distinction matters because it changes urgency, treatment pathways, and how the ECG is interpreted at the bedside. Both conditions sit within the acute coronary syndrome spectrum, and both can be dangerous. However, they do not look the same on the ECG, they do not always reflect the same degree of coronary occlusion, and they are not managed with the same immediate timetable.
In simple terms, STEMI is the pattern that should make you think about immediate reperfusion. NSTEMI is the pattern that still represents myocardial infarction but usually requires rapid risk stratification, serial ECGs, troponin interpretation, and timely invasive planning rather than automatic emergency activation for reperfusion. The challenge for beginners is that NSTEMI can be subtle, the first ECG may be nondiagnostic, and troponin must be interpreted in context rather than as a stand-alone answer.
What STEMI and NSTEMI have in common
Both STEMI and NSTEMI are forms of acute myocardial infarction. That means both require acute myocardial injury, shown by a rise and/or fall in cardiac troponin with at least one value above the 99th percentile upper reference limit, together with evidence of acute myocardial ischaemia. In other words, they are both infarctions, not merely chest pain syndromes. Both can produce complications such as arrhythmia, heart failure, cardiogenic shock, and death if missed or treated too late.
Both also sit within the broader acute coronary syndrome framework. Acute coronary syndrome includes unstable angina, NSTEMI, and STEMI. Unstable angina causes ischaemic symptoms without biomarker-defined infarction. NSTEMI and STEMI both involve myocardial necrosis, which is why troponin becomes elevated in each.
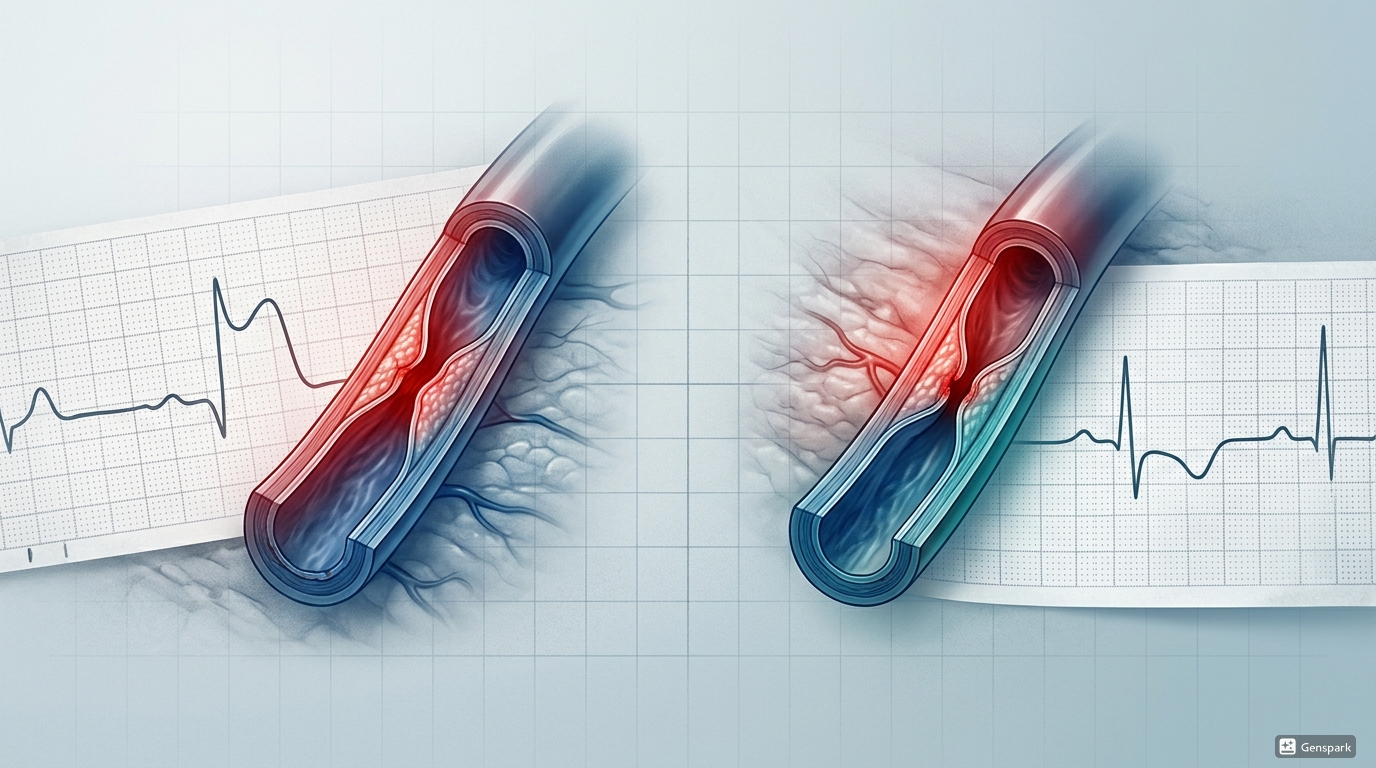
The main difference in pathophysiology
The traditional teaching is that STEMI usually reflects a sudden complete coronary occlusion producing transmural ischaemia or infarction, while NSTEMI usually reflects subtotal or intermittent occlusion producing subendocardial infarction. This teaching is useful because it helps explain the ECG pattern: transmural injury is more likely to generate ST elevation, whereas subendocardial injury more often causes ST depression or T-wave inversion.
However, clinical reality is not always so neat. Some dangerous coronary occlusions do not meet classic STEMI criteria, and some patients without persistent ST elevation may still have a severely threatened myocardium. That is why ECG interpretation should never be reduced to pattern memorisation alone. The ECG must always be read together with symptoms, timing, haemodynamic status, and serial changes.

Why the ECG comes first
In suspected acute coronary syndrome, the 12-lead ECG is the first critical test because it guides time-sensitive action. Current guidance emphasises that an ECG should be obtained and interpreted within 10 minutes of presentation in suspected ACS. This matters most in STEMI, because the diagnosis can trigger immediate reperfusion therapy without waiting for troponin confirmation. If a patient has ischaemic symptoms and the ECG shows new ST elevation in contiguous leads, the tracing may be enough to activate the reperfusion pathway.
The opposite pitfall is assuming a nondiagnostic ECG excludes myocardial infarction. It does not. NSTEMI may present with ST depression, T-wave inversion, transient changes, or even an initially normal ECG. Dynamic changes may evolve with time, so repeat ECGs are essential when symptoms continue or recur.

How STEMI looks on the ECG
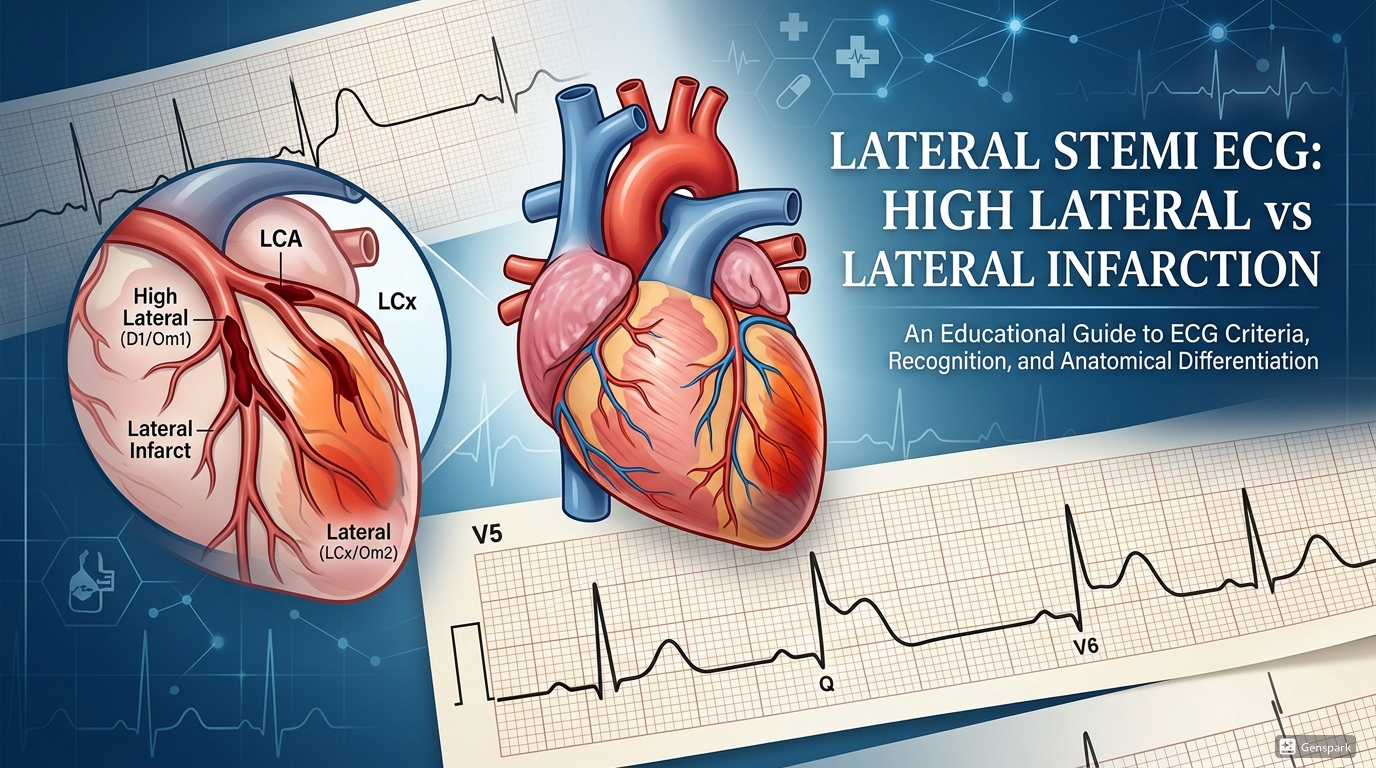
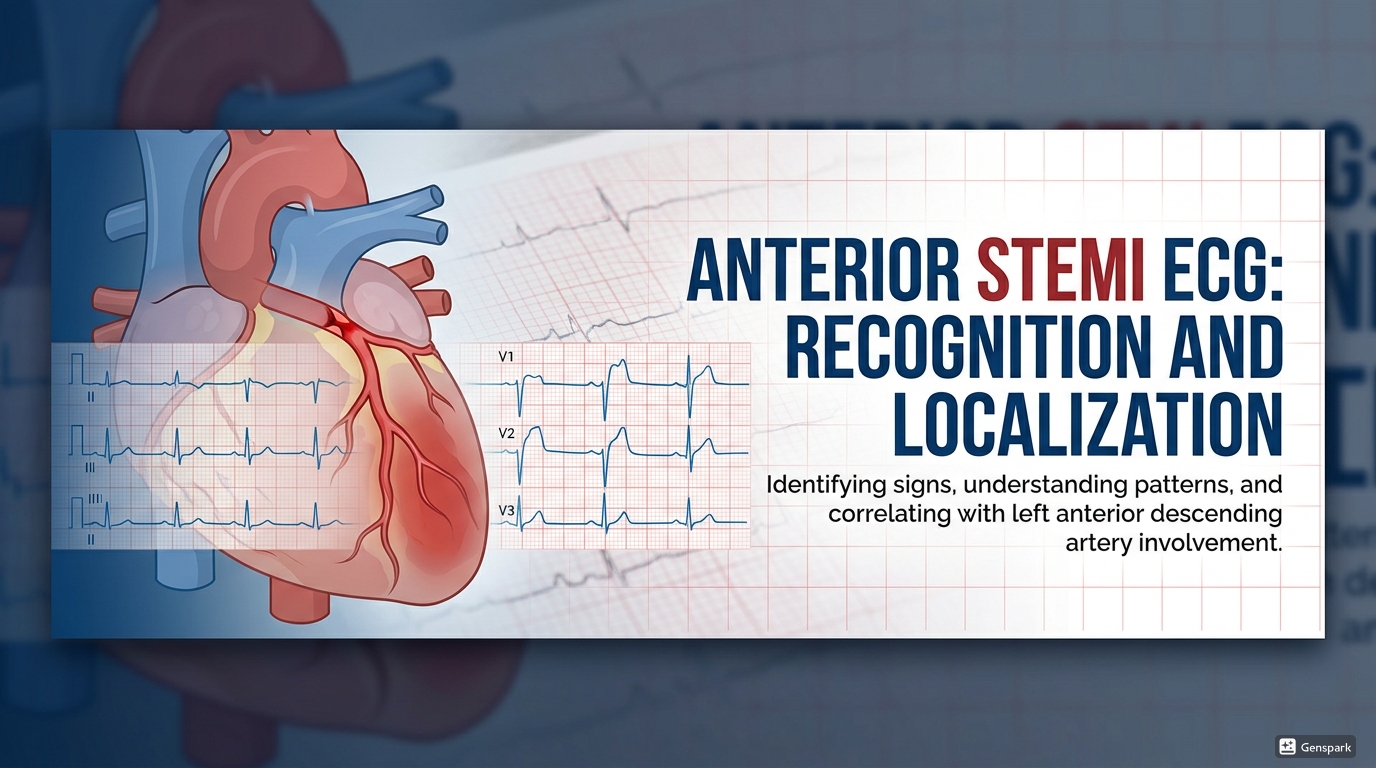
STEMI is classically recognised by persistent ST-segment elevation in two or more contiguous leads in a patient with compatible ischaemic symptoms. In practice, the ECG may also show reciprocal ST depression in opposite territories, hyperacute T waves early on, and later pathological Q waves depending on timing. The exact leads involved help localise the infarct territory: anterior, inferior, lateral, septal, or combinations of these.
For junior doctors, the safest habit is to ask three questions. First, is there definite ST elevation? Second, are the affected leads contiguous? Third, are there reciprocal changes that strengthen the impression of acute infarction? STEMI can sometimes be subtle, especially in inferior infarction, so careful lead-by-lead review is important.

How NSTEMI looks on the ECG
NSTEMI does not show persistent ST-segment elevation at presentation. Instead, common ECG findings include horizontal or downsloping ST depression, T-wave inversion, or both. Some patients may have transient ST elevation that resolves, and others may present with nonspecific or initially normal tracings. That is why NSTEMI is often more difficult for beginners: the ECG changes can be less dramatic, less specific, and more dependent on serial comparison.
A useful practical point is that NSTEMI is not diagnosed by ECG alone. The ECG raises suspicion, but the diagnosis depends on biomarker evidence of myocardial necrosis together with clinical evidence of ischaemia. This means the ECG and troponin results must be interpreted as a pair rather than in isolation.

The role of troponin in STEMI vs NSTEMI
Troponin is elevated in both STEMI and NSTEMI because both involve myocardial necrosis. The difference is how urgently the clinician must act before that result returns. In STEMI, a classic ECG in the right clinical context should drive reperfusion decisions immediately. Waiting for troponin can waste myocardium. In NSTEMI, troponin becomes central because the ECG does not provide the same immediate reperfusion signal. Serial troponin testing helps confirm infarction, distinguish acute injury from chronic elevation, and support risk stratification.
The universal definition reminds us that troponin above the 99th percentile indicates myocardial injury, not automatically myocardial infarction. To diagnose MI, there must also be evidence of ischaemia. This is especially important in NSTEMI work-up because positive troponin can also occur in myocarditis, pulmonary embolism, tachyarrhythmia, sepsis, heart failure, and chronic kidney disease.
STEMI vs NSTEMI vs unstable angina
Students often confuse NSTEMI with unstable angina. The easiest way to separate them is to remember that unstable angina does not meet biomarker criteria for infarction. Symptoms may be similar, and the ECG can also show transient ST depression or T-wave inversion, but troponin does not show the rise and/or fall pattern required for myocardial infarction. NSTEMI, by contrast, has biomarker evidence of myocardial necrosis. STEMI also has biomarker evidence of necrosis, but with the classic ST-elevation pattern on ECG.
How management urgency differs
The biggest practical difference is urgency of reperfusion. STEMI is a reperfusion emergency. The system should move quickly toward primary PCI when available because ongoing coronary occlusion threatens a large amount of myocardium. NSTEMI is still urgent, but the pathway is usually built around anti-thrombotic therapy, serial ECGs, serial troponin testing, risk assessment, and early invasive evaluation according to clinical severity and risk profile rather than automatic immediate reperfusion for every patient.
That said, NSTEMI can still be very high risk. Persistent chest pain, haemodynamic instability, recurrent dynamic ECG changes, ventricular arrhythmia, heart failure, or cardiogenic shock should make clinicians escalate quickly. Beginners should avoid the false reassurance that “no ST elevation” means “not urgent.”
A practical bedside approach for junior doctors
When you assess possible myocardial infarction, work through the following sequence:
- Is the patient having symptoms compatible with acute myocardial ischaemia?
- Has a 12-lead ECG been obtained and interpreted within 10 minutes?
- Does the ECG show persistent ST elevation in contiguous leads or another clear reperfusion pattern?
- If there is no ST elevation, are there ST depressions, T-wave inversions, or dynamic ECG changes that support NSTEMI?
- What do the troponin results show, and is there a rise and/or fall pattern?
- Could another condition explain the symptoms or the troponin elevation?
- Does the patient need immediate reperfusion, urgent senior review, or high-risk NSTEMI escalation?
This structured approach reduces cognitive overload and helps distinguish the bedside priorities of STEMI from the more investigative but still urgent pathway of NSTEMI.
Common mistakes to avoid
- Waiting for troponin to confirm an obvious STEMI before escalating reperfusion care.
- Assuming a normal or nondiagnostic first ECG rules out NSTEMI.
- Calling every positive troponin an NSTEMI without looking for non-ischaemic causes of myocardial injury.
- Missing subtle or inferior ST elevation because the tracing does not look dramatic at first glance.
- Treating “no ST elevation” as “low risk” despite ongoing pain or haemodynamic instability.
Frequently asked questions
Is STEMI always more dangerous than NSTEMI?
Not automatically. STEMI usually demands more immediate reperfusion because of the risk of full coronary occlusion, but NSTEMI can also be severe and high risk depending on the clinical picture and coronary anatomy.
Can troponin be elevated in both STEMI and NSTEMI?
Yes. Both are myocardial infarctions and both usually cause troponin elevation. The ECG pattern and clinical pathway differ more than the fact of biomarker release.
Can NSTEMI have a normal ECG initially?
Yes. The first ECG can be normal or nonspecific. That is why repeat ECGs and serial troponins are so important in suspected ACS.
Does ST elevation always mean STEMI?
No. Pericarditis, early repolarisation, left ventricular aneurysm, and other conditions can cause ST elevation. Interpretation depends on symptoms, lead pattern, reciprocal changes, and clinical context.
What is the simplest exam definition of NSTEMI?
Myocardial infarction with elevated troponin and evidence of ischaemia, but without persistent ST-segment elevation on the presenting ECG.
Key takeaways
- Both STEMI and NSTEMI are acute myocardial infarctions within the ACS spectrum.
- STEMI usually shows persistent ST elevation and typically triggers immediate reperfusion therapy.
- NSTEMI does not show persistent ST elevation and often presents with ST depression, T-wave inversion, or dynamic but subtle changes.
- Troponin is elevated in both conditions, but STEMI management should not wait for biomarker confirmation when the ECG is diagnostic.
- A nondiagnostic first ECG does not rule out NSTEMI, so serial ECGs and serial troponins matter.
- Clinical context, ECG findings, and biomarker patterns should always be interpreted together.
References
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction.
- MSD Manual Professional Edition. Overview of Acute Coronary Syndromes (ACS).
- European Society of Cardiology. 2023 ESC Guidelines for the management of acute coronary syndromes.
- 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Diagnosis and Risk Classification of Acute Coronary Syndromes.
Included image files
- Featured thumbnail hero image
- STEMI vs NSTEMI pathophysiology illustration
- STEMI ECG image
- NSTEMI ECG image
- ACS evaluation flowchart