Acute Coronary Syndrome Explained for Medical Students and Junior Doctors
Description: A practical guide to acute coronary syndrome covering unstable angina, NSTEMI, STEMI, ECG changes, troponin, early management, and common clinical pitfalls.

|
Quick answer: Acute coronary syndrome (ACS) is the clinical spectrum caused by sudden reduction in coronary blood flow, usually after plaque rupture and thrombus formation. It includes unstable angina, NSTEMI, and STEMI. In practice, junior clinicians should think of ACS as a time-critical diagnosis built from symptoms, a 12-lead ECG, and serial high-sensitivity troponin testing. STEMI usually requires immediate reperfusion, while NSTEMI and unstable angina demand prompt risk stratification, antithrombotic therapy, and careful monitoring. |
Acute chest pain is one of the commonest reasons patients present to the emergency department, acute medical unit, or coronary care service. For medical students and junior doctors, few topics are more important than acute coronary syndrome. It is common, dangerous, and highly testable. It also rewards a structured approach. When you understand what ACS is, why it happens, and how it appears on the ECG and in blood tests, decision-making becomes much clearer.
At the bedside, ACS is not just a cardiology label. It is a working diagnosis that changes what happens next: the urgency of ECG acquisition, how rapidly troponin is sent, which antiplatelet and anticoagulant treatments are considered, and whether the patient needs immediate transfer for coronary angiography or percutaneous coronary intervention. For junior doctors, the main challenge is not memorising definitions; it is recognising the syndrome early enough to avoid missing a dangerous infarction.
What is acute coronary syndrome?
Acute coronary syndrome describes myocardial ischaemia caused by an abrupt decrease in blood flow through a coronary artery. In most cases, the underlying event is rupture or erosion of an atherosclerotic plaque followed by platelet activation and thrombus formation. The resulting obstruction may be partial, intermittent, or complete. The degree and duration of occlusion determine the clinical picture.
ACS is usually divided into three entities. Unstable angina causes myocardial ischaemia without detectable myocardial necrosis, so troponin does not rise above the diagnostic threshold. Non-ST elevation myocardial infarction (NSTEMI) causes myocardial necrosis but without persistent ST-segment elevation on the ECG. ST-elevation myocardial infarction (STEMI) is usually associated with a persistent occlusive event and classic ST-segment elevation requiring urgent reperfusion. These categories help clinicians triage risk and treatment, even though the underlying biology may overlap.

Textbook-style overview of the ACS spectrum: unstable angina, NSTEMI, and STEMI.
Why ACS matters so much in early clinical practice
The first hours matter. A missed or delayed diagnosis can mean a larger infarct, cardiogenic shock, malignant arrhythmia, mechanical complications, or death. That is why suspected ACS is approached as a time-sensitive pathway rather than a routine ward problem. The first tasks are simple but urgent: assess airway, breathing, and circulation; obtain a focused history; record a 12-lead ECG rapidly; check vital signs; and arrange serial cardiac biomarkers. If the patient has ongoing ischaemic pain, haemodynamic instability, or clear STEMI features, escalation should be immediate.
For learners, one helpful principle is this: chest pain is not equal to ACS, but ACS must stay near the top of the differential until it is safely excluded. A normal initial ECG does not completely rule out NSTEMI, and a single normal troponin early after symptom onset may also be misleading. Serial assessment is central.
The pathophysiology in simple terms
Most ACS events begin with an unstable atherosclerotic plaque. When that plaque ruptures or erodes, the subendothelial contents trigger platelet adhesion and activation. A thrombus forms on top of the plaque. If the thrombus severely limits or completely blocks coronary flow, the myocardium downstream becomes ischaemic. If ischaemia is prolonged, cardiomyocytes die and troponin enters the circulation.
A completely occlusive thrombus is more likely to produce transmural ischaemia and ST-segment elevation, which is the classic STEMI pattern. Partial or dynamic obstruction is more likely to produce subendocardial ischaemia, which commonly appears as ST depression or T-wave inversion and fits the NSTEMI pattern. However, real clinical life is messier than simplified diagrams. Some dangerous occlusive infarctions may not show classic STEMI criteria, so clinicians must always interpret the ECG in context.
How patients with ACS present
The classic symptom is central chest discomfort described as pressure, heaviness, squeezing, or tightness. Pain may radiate to the left arm, both arms, neck, jaw, back, or epigastrium. Associated symptoms include diaphoresis, nausea, vomiting, dyspnoea, palpitations, presyncope, and an overwhelming sense of illness. Some patients, especially older adults, women, and people with diabetes, may present atypically with breathlessness, fatigue, collapse, or epigastric discomfort rather than textbook chest pain.
History still matters. Ask about the character of pain, duration, triggers, relation to exertion, and whether it settles with rest or nitrates. Clarify cardiovascular risk factors such as smoking, hypertension, diabetes, dyslipidaemia, chronic kidney disease, prior coronary disease, and family history. But remember that risk factors support a diagnosis; they do not make it. A young patient can still have ACS, and a patient with many risk factors can have non-cardiac pain.
The three major ACS categories
1. Unstable angina
Unstable angina is myocardial ischaemia without measurable myocardial necrosis. Symptoms may occur at rest, become more frequent, last longer than previous angina episodes, or be more severe than usual. Troponin remains below the infarction threshold. The ECG may show ST depression, T-wave inversion, or can even be normal. Although unstable angina is less common in the high-sensitivity troponin era, it remains an important diagnosis because these patients are still at meaningful risk of future infarction.
2. NSTEMI
NSTEMI means there is myocardial injury with a rise and/or fall in cardiac troponin above the diagnostic threshold, together with clinical evidence of ischaemia, but without persistent ST-segment elevation on the ECG. ECG findings often include horizontal or downsloping ST depression, transient ST elevation, or T-wave inversion, but the initial ECG may be nondiagnostic. Many junior clinicians miss the importance of serial ECGs in this group.
3. STEMI
STEMI is the ACS pattern most clinicians recognise fastest because the ECG typically shows persistent ST-segment elevation in contiguous leads. It usually reflects an acute occlusive coronary event and demands immediate reperfusion therapy, most commonly primary PCI when available within the recommended system timelines. Delays matter because “time is muscle”: the longer the occlusion persists, the larger the infarct size and the worse the clinical outcome.

Realistic unannotated 12-lead ECG example with a STEMI pattern.

Realistic unannotated 12-lead ECG example with an NSTEMI/ischaemia pattern.

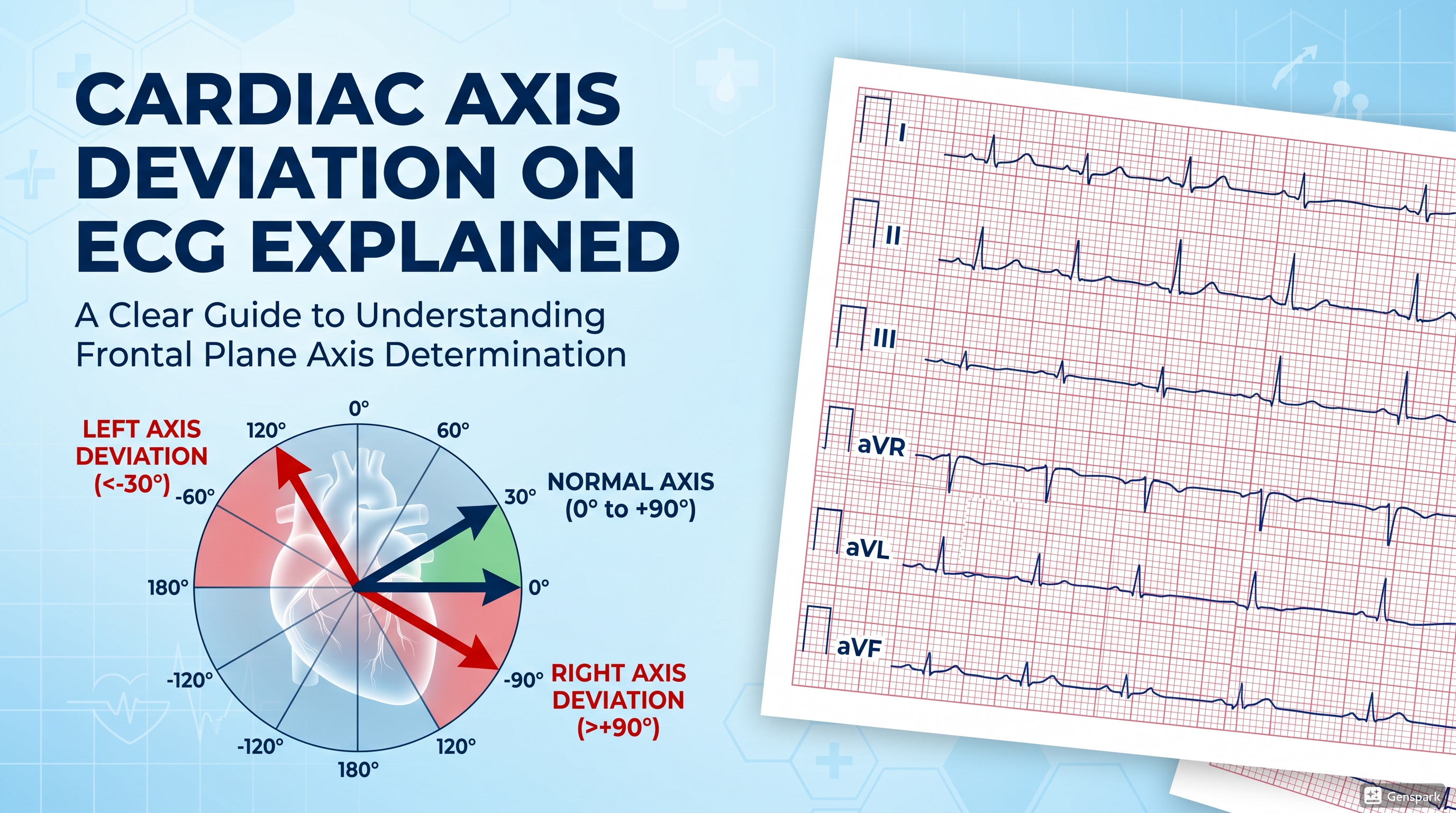
The ECG approach every junior doctor should use
When ACS is suspected, the ECG should be reviewed systematically rather than by vague pattern recognition alone. First, confirm calibration and scan for rhythm, rate, and conduction abnormalities. Next, look for obvious ST-segment elevation in contiguous leads and ask whether there are reciprocal changes. Then search for ST depression, T-wave inversion, hyperacute T waves, new bundle branch block, or dynamic changes compared with prior tracings. If the ECG is not diagnostic but symptoms persist, repeat the ECG. Many important changes evolve over time.
A useful beginner structure is: Is there ST elevation? If yes, in which contiguous leads? Do the involved leads suggest an inferior, anterior, septal, or lateral territory? Is there reciprocal depression elsewhere? If there is no persistent ST elevation, are there ischaemic changes that support NSTEMI or unstable angina? Finally, does the clinical picture match what you are seeing, or could this be a mimic such as pericarditis, left ventricular hypertrophy, bundle branch block, paced rhythm, or lead misplacement?
What troponin actually tells you
Cardiac troponin is the preferred biomarker for myocardial injury. High-sensitivity assays have improved early detection, but they also require careful interpretation. A raised troponin does not automatically mean type 1 myocardial infarction due to plaque rupture. Troponin can rise in myocarditis, tachyarrhythmia, heart failure, renal dysfunction, pulmonary embolism, sepsis, and other critical illness. The diagnosis of acute MI therefore requires both a rise and/or fall in troponin and evidence of myocardial ischaemia from the history, ECG, imaging, or angiography.
For junior doctors, the mistake is often to use troponin in isolation. Instead, think in layers: symptoms, ECG, serial troponin pattern, haemodynamic status, and alternative diagnoses. Troponin confirms injury; it does not replace clinical reasoning.
Early management priorities in suspected ACS
The first steps in management are stabilisation and rapid diagnosis. Assess ABCDE, establish monitoring, obtain intravenous access, and treat immediate threats such as hypoxia, hypotension, pulmonary oedema, or arrhythmia. Give analgesia when needed, but keep reassessing because worsening pain can signal ongoing ischaemia. Aspirin is a cornerstone in most ACS pathways unless contraindicated. Further antiplatelet or anticoagulant therapy depends on whether the patient is managed as STEMI or NSTE-ACS and on local protocols.
In STEMI, the priority is reperfusion. In NSTEMI or unstable angina, the next steps depend on risk profile, ECG findings, biomarker pattern, ongoing symptoms, and haemodynamic stability. Some patients need urgent angiography; others can undergo an early invasive strategy after risk stratification. Junior doctors do not need to decide every detail alone, but they do need to recognise the sick patient early and call for senior help promptly.
Common complications you should watch for
ACS can deteriorate quickly. Electrical complications include ventricular tachycardia, ventricular fibrillation, atrial fibrillation, and bradyarrhythmias. Haemodynamic complications include acute heart failure, pulmonary oedema, and cardiogenic shock. Mechanical complications, although less common in the reperfusion era, remain exam favourites and clinical emergencies: papillary muscle rupture causing acute mitral regurgitation, ventricular septal rupture, and free-wall rupture with tamponade. Recurrent chest pain, hypotension, new murmurs, rising lactate, or abrupt pulmonary oedema should never be ignored.
A practical bedside framework for learners
If you are asked to assess a possible ACS patient, use this mental checklist:
- Is the patient stable or unstable right now?
- What is the nature of the chest pain or equivalent symptom?
- Has a 12-lead ECG been done and repeated if needed?
- Are there STEMI features, ischaemic ST depression, or dynamic T-wave changes?
- What do the initial and repeat troponins show?
- Could there be another dangerous diagnosis such as aortic dissection, pulmonary embolism, or pericarditis?
- Does this patient need urgent senior review, cardiology input, or transfer for reperfusion?
This framework keeps the assessment grounded. It also reduces the chance that you will focus too early on a single blood test or a vague description of pain while missing the wider clinical picture.
Common mistakes in ACS assessment
- Assuming a normal first ECG rules out ACS.
- Treating troponin as a yes/no test for myocardial infarction without considering alternative causes of injury.
- Failing to repeat the ECG when symptoms continue or recur.
- Underestimating atypical presentations in older adults, women, and patients with diabetes.
- Delaying escalation in a patient with ongoing pain, haemodynamic instability, or clear STEMI features.
- Ignoring reciprocal changes or subtle ischaemic patterns because the tracing does not look dramatic.
Frequently asked questions
Can a patient have ACS with a normal ECG?
Yes. A single normal ECG does not exclude ACS, especially NSTEMI or unstable angina. Repeat ECGs and serial troponins are essential when the history is concerning.
Does every elevated troponin mean myocardial infarction?
No. Troponin indicates myocardial injury, not always type 1 MI. Interpretation depends on the rise/fall pattern and whether there is evidence of ischaemia.
Is unstable angina still a real diagnosis in the high-sensitivity troponin era?
Yes, although it is diagnosed less often than before. Patients may have ischaemic symptoms without a diagnostic troponin rise yet still carry important short-term risk.
What is the main difference between STEMI and NSTEMI at the bedside?
STEMI usually triggers immediate reperfusion because it implies an acute occlusive event with persistent ST elevation. NSTEMI requires urgent but usually less immediate invasive planning guided by risk stratification.
Why are serial ECGs important?
Because ischaemic changes can evolve. A nondiagnostic first ECG can become clearly abnormal later, especially if chest pain continues.
Key takeaways
- ACS is a spectrum that includes unstable angina, NSTEMI, and STEMI.
- The usual mechanism is plaque disruption with thrombus formation and reduced coronary blood flow.
- STEMI is recognised by persistent ST-segment elevation and generally requires urgent reperfusion.
- NSTEMI depends on troponin rise/fall plus clinical evidence of ischaemia, often with ST depression or T-wave inversion rather than ST elevation.
- A normal initial ECG or a single early troponin does not safely exclude ACS.
- Serial ECGs, serial troponins, and clinical context are the foundations of safe assessment.
- Junior doctors should escalate early when symptoms, ECG changes, or haemodynamic instability suggest high risk.
References
- European Society of Cardiology. 2023 ESC Guidelines for the management of acute coronary syndromes.
- MSD Manual Professional Edition. Overview of Acute Coronary Syndromes (ACS).
- American Heart Association. Acute Coronary Syndrome.
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction. Circulation.
- American Heart Association / ACC / ACEP / NAEMSP / SCAI. Guideline for the diagnosis and risk classification of acute coronary syndromes.