ECG Leads Explained: What Each Lead Looks At

Quick Answer
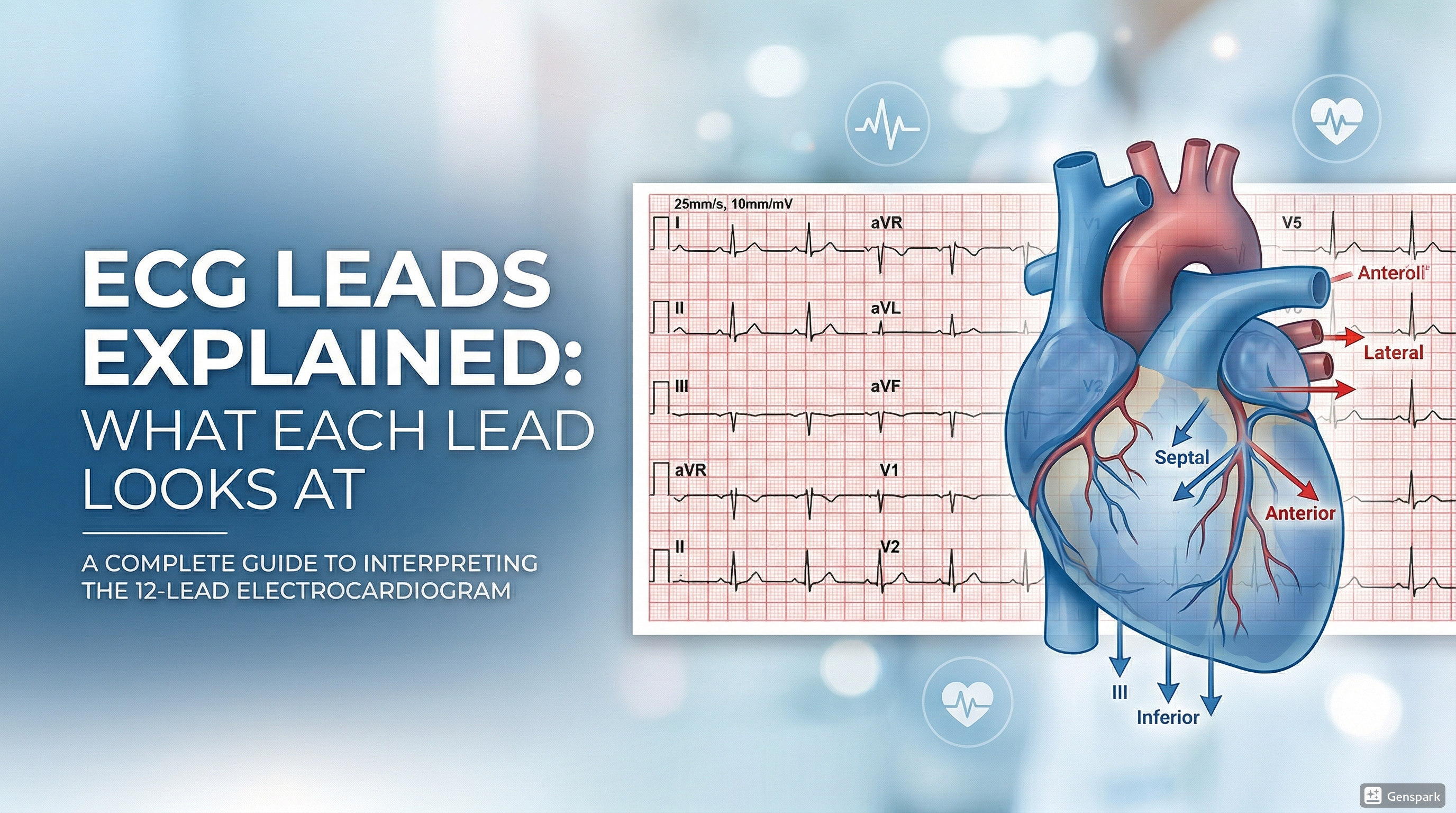
A 12-lead ECG does not give 12 different heartbeats. It gives 12 different views of the same electrical event. The limb leads look at the heart in the frontal plane, while the chest leads look at it in the horizontal plane. Inferior leads are II, III, and aVF; lateral leads are I, aVL, V5, and V6; septal leads are V1 and V2; and anterior leads are V3 and V4. Understanding what each lead looks at is essential for localizing ischemia, infarction, conduction abnormalities, and chamber strain.
Introduction
One of the biggest turning points in learning ECG interpretation is understanding that each lead is simply a different camera angle on the same heart. Many students memorize lead names early but still feel confused when someone says, “There is ST elevation in the inferior leads” or “The septal leads look abnormal.” That confusion usually comes from not having a clear mental model of what the leads actually represent.
This article explains ECG leads in a step-by-step, clinically practical way. The goal is not just to help you pass an exam. It is to help you look at a 12-lead ECG and immediately know which leads belong together, what region of the heart they mainly reflect, and why this matters in everyday cardiology and acute care.
For medical students and junior doctors, this is foundational knowledge. Once you understand lead viewpoints, topics such as myocardial infarction localization, bundle branch block, axis deviation, ventricular hypertrophy, and even lead misplacement become much easier to understand.
What Is the Difference Between an Electrode and a Lead?
This is the first concept that clears up a lot of confusion. An electrode is the physical sticker or contact placed on the patient. A lead is the electrical view produced from those electrodes. In other words, the electrodes collect the signal, and the leads are the perspectives generated from that signal.
That is why a standard 12-lead ECG does not require 12 separate chest stickers. It uses limb and chest electrodes to generate 12 views of cardiac electrical activity. The trace on the paper is a set of viewpoints, not 12 separate recording machines.
How Many Electrodes Are Used in a 12-Lead ECG?
A standard 12-lead ECG is usually obtained using 10 electrodes: four limb electrodes and six chest electrodes. From those 10 electrodes, the machine generates 12 leads.
- Limb electrodes: right arm, left arm, right leg, left leg
- Chest electrodes: V1, V2, V3, V4, V5, V6
The right leg electrode is usually a ground rather than a lead that provides a diagnostic view. The remaining electrodes are used to create the limb leads and the precordial leads.

The Two Big Viewpoints: Frontal Plane and Horizontal Plane
The simplest way to organize ECG leads is to divide them into the two planes they observe.
Frontal plane
The limb leads view the heart from the frontal plane. These are leads I, II, III, aVR, aVL, and aVF. They help you understand how the electrical impulse is moving up, down, left, or right across the body when viewed from the front.
Horizontal plane
The precordial or chest leads view the heart from the horizontal plane. These are V1 to V6. They move across the chest from right parasternal to left lateral positions and are especially useful for seeing septal, anterior, and lateral ventricular activity.
If you remember only one thing at first, remember this: limb leads tell you what is happening in the frontal plane, while chest leads tell you what is happening in the horizontal plane.
[Image unavailable] Overview of the 12-lead ECG viewpoints around the heart.
The Limb Leads Explained
The limb leads are I, II, III, aVR, aVL, and aVF. Together they give six frontal-plane views of the heart.
Lead I
Lead I looks from the right arm toward the left arm. In simple teaching language, it gives a leftward lateral view of the heart.
Lead II
Lead II looks from the right arm toward the left leg. This lead is especially useful because normal sinus P waves are often upright here, and it also contributes to the inferior lead group.
Lead III
Lead III looks from the left arm toward the left leg. Like lead II, it belongs to the inferior lead group.
aVR
aVR looks from the right arm. Beginners often ignore aVR, but it is still useful. In a normal ECG, many waveforms are negative in aVR because the main depolarization vector travels away from the right shoulder.
aVL
aVL looks from the left arm and gives a high lateral view of the heart. It is often grouped with lead I as a lateral lead.
aVF
aVF looks upward from the foot or inferior direction. It is part of the inferior lead group together with II and III.
A practical beginner summary is this: II, III, and aVF look inferiorly; I and aVL look laterally; and aVR looks from the right shoulder.
The Precordial Leads Explained
The chest leads V1 to V6 are placed across the anterior chest wall. They view the heart in the horizontal plane, moving from the right side of the sternum toward the left lateral chest.
V1
V1 is placed in the fourth intercostal space at the right sternal border. It mainly provides a septal or right-sided anterior view. It is useful for assessing bundle branch block patterns and right ventricular signals.
V2
V2 is placed in the fourth intercostal space at the left sternal border. Together with V1, it mainly reflects septal activity.
V3
V3 is positioned between V2 and V4. It begins to transition from septal to anterior viewpoints.
V4
V4 is placed in the fifth intercostal space at the midclavicular line. It is classically considered an anterior lead.
V5
V5 is at the same horizontal level as V4, in the anterior axillary line. It gives a lateral view of the left ventricle.
V6
V6 is at the same level as V4 and V5, in the midaxillary line. It is also a lateral lead.
A simple mental picture is that the precordial leads march across the front and side of the chest, moving from septal views on the right to lateral views on the left.
Standard Chest Lead Positions You Should Know
- V1: 4th intercostal space, right sternal border
- V2: 4th intercostal space, left sternal border
- V3: midway between V2 and V4
- V4: 5th intercostal space, midclavicular line
- V5: same horizontal level as V4, anterior axillary line
- V6: same horizontal level as V4, midaxillary line
Incorrect placement can significantly alter the ECG appearance. For example, placing V1 and V2 too high can create misleading patterns and can mimic pathology. That is why learning lead placement is not just a technical issue; it is part of interpretation.
Which Leads Belong Together?
Grouping leads into anatomic territories is one of the most useful habits in ECG reading. When contiguous leads show similar abnormalities, they often point to a localized process such as ischemia, infarction, or ventricular strain.
- Inferior leads: II, III, aVF
- High lateral / lateral leads: I, aVL, V5, V6
- Septal leads: V1, V2
- Anterior leads: V3, V4
Some clinicians combine these groups slightly differently, but this framework is very useful for beginners and works well in daily practice. Inferior changes suggest inferior wall involvement; anterior changes suggest anterior wall involvement; lateral changes suggest lateral wall involvement.

What Each Lead Group Looks At Clinically
Inferior leads
Leads II, III, and aVF mainly reflect the inferior wall of the left ventricle. If these leads show ST elevation in a patient with ischemic symptoms, think about an inferior myocardial infarction pattern.
Lateral leads
Leads I, aVL, V5, and V6 mainly reflect the lateral wall of the left ventricle. Lateral abnormalities may be seen in lateral infarction, left ventricular hypertrophy with strain, and other repolarization disorders.
Septal leads
V1 and V2 are often referred to as the septal leads because they primarily face the interventricular septum. They are also important in bundle branch blocks and in assessing R-wave progression.
Anterior leads
V3 and V4 mainly reflect the anterior wall of the left ventricle. These leads are especially important when assessing anterior ischemia or infarction.
Why aVR Matters More Than Many Beginners Think
aVR is often neglected because the waveform is frequently negative in normal tracings. However, it is still useful. aVR can support recognition of lead misplacement, broad ischemic patterns, and certain tachyarrhythmias or conduction abnormalities. You do not need to master all advanced aVR uses immediately, but you should avoid thinking of it as a meaningless lead.
How Lead Knowledge Helps You Read ECGs Faster
Understanding lead groups makes the 12-lead ECG far less intimidating. Instead of looking at twelve separate traces as isolated lines, you begin to see meaningful clusters. If II, III, and aVF all show the same abnormality, that is more informative than seeing a single odd-looking beat in only one lead. If V1 and V2 behave differently from V5 and V6, that pattern may help you recognize conduction disease or ventricular hypertrophy.
This is also why ECG localization works. When multiple neighboring leads become abnormal together, they often reflect a real anatomic process rather than artifact or random variation.
Common Mistakes Beginners Make With ECG Leads
A very common mistake is confusing lead placement with the anatomic surface of the heart. A lead does not directly photograph a wall of the heart in the same way an imaging test does. Instead, it records electrical activity from a specific viewpoint. The territory labels such as inferior, anterior, and lateral are useful clinical simplifications, not perfect anatomical photographs.
Another common mistake is forgetting that abnormal electrode placement can create a misleading ECG. Limb lead reversal, misplaced V1 and V2, or poor skin contact can all produce patterns that look pathological. If the ECG seems strange, always consider whether the leads were placed correctly.
Students also sometimes memorize the chest lead names but forget the actual positions. That becomes a problem later when trying to understand R-wave progression, bundle branch blocks, or right ventricular patterns.
A Simple Way to Memorize the Leads
One practical approach is to memorize the groups before memorizing every detail.
- Inferior = II, III, aVF
- Lateral = I, aVL, V5, V6
- Septal = V1, V2
- Anterior = V3, V4
Then learn the chest lead positions physically on the torso. Finally, connect the viewpoint to the clinical use. Once you do this repeatedly, the 12-lead ECG becomes much more logical.
FAQ
What are the 12 leads of an ECG?
The 12 leads are I, II, III, aVR, aVL, aVF, and V1 to V6.
How many electrodes are used in a 12-lead ECG?
A standard 12-lead ECG typically uses 10 electrodes: four limb electrodes and six chest electrodes.
Which leads are inferior on ECG?
The inferior leads are II, III, and aVF.
Which leads are lateral on ECG?
The lateral leads are I, aVL, V5, and V6.
Which leads are septal and anterior?
V1 and V2 are classically septal leads, while V3 and V4 are classically anterior leads.
Why is aVR important?
aVR is important because it provides a rightward viewpoint and can help with recognition of certain ischemic, conduction, and lead-placement patterns.
Key Takeaways
A 12-lead ECG gives 12 different views of the same cardiac electrical activity. The limb leads look at the frontal plane, and the chest leads look at the horizontal plane. Inferior leads are II, III, and aVF; lateral leads are I, aVL, V5, and V6; septal leads are V1 and V2; and anterior leads are V3 and V4.
For medical students and junior doctors, mastering the lead groups is one of the fastest ways to improve ECG interpretation. Once you know what each lead looks at, patterns such as infarction localization, repolarization abnormalities, and conduction changes become easier to recognize and explain.
References
- American Heart Association. Electrocardiogram (EKG or ECG).
- American Heart Association. 12 Lead Placement.
- LITFL. ECG Lead Positioning.
- ECG Waves. Electrodes, Limb Leads, Chest (Precordial) Leads and the 12-Lead ECG.